The fact that nobody is talking about Secret’s new commercials pisses me off
This makes me so happy ☺️
Yesssss😭 I damn near cried
I LOVE THIS OMFG
YOOOOOOOOOOO THATS AMAZING!!!!!
Can someone help me understand I wanna cry to ..I feel something went over my head
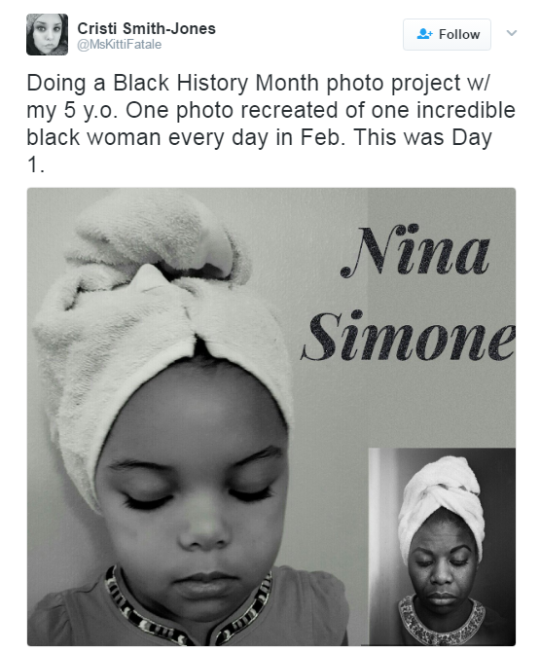
The woman in the bathroom is trans and is scared that if she comes out of the stall the women that walked in will insult or harass her. but when she comes out they compliment her on her dress instead. The add ends with saying “stress tested for women.” It means Secret is including trans women in their definition of women.
I have reblogged this three times now, each one mentioning the fact that Secret not only included a trans woman, but that they /had the other women compliment her dress and treat her with respect/. I will reblog this every time I see it because it’s so important. More companies should involve trans people in their marketing – we do exist. Props to Secret for getting in on this movement. It makes me really happy to see more of the trans community represented in daily television.
1. Progesterone: not for everyone, but for many people it may increase
sex drive and WILL make your boobs bigger. Also effects mood in ways
that many find positive (but some find negative). Most doctors won’t
prescribe this to you unless you ask. Most trans girls I know swear by
it.
2. Injectible estrogen: is
more effective than pill or patch form. Get on it if you can bear
needles bc you will see more effects more quickly.
3. Estradiol
Cypionate: There is currently a shortage of injectible estradiol
valerate. There is no shortage of estradiol cypionate. Functionally they
do the same shit.
4. Bicalutamide: This is an anti-androgen that
has almost none of the side-effects of spironolactone or finasteride.
The girls I know who are on it are evangelical about it.
Are there HRT medications that don’t increase blood clot risk? I’m already at risk because of my blood pressure, and my doctor won’t prescribe HRT that increases clot risk while I’m on the medication – and I may never not be on the medication.
Absolutely.
The concerns surrounding venous thromboembolic events as a side-effect of hormone replacement therapy can mostly be traced back to one particular study known as the Women’s Health Initiative. This study was an enormous undertaking which, unfortunately, demonstrated significant adverse effects of the hormone therapies studied. As a result of this the use of hormone replacement therapy in postmenopausal cis women was dramatically reduced as the medical community began to question whether or not the therapy caused more harm than good.
Naturally, trans women have been suffering from this fall-out ever since.
What physicians seem to fail to recognize is that the study examined a very specific hormone regimen which was, arguably, outmoded at the time the study was conducted: It examined the use of conjugated equine estrogen (Premarin) with or without the use of medroxyprogesterone acetate. Neither of these drugs is regularly used for the treatment of transgender women.
The estrogen most commonly used to treat transgender women nowadays is 17β-estradiol either in pill form or in the form of a sticky patch that you apply to your skin. Esters of estrogen (e.g. estradiol valerate) are also sometimes used either in a pill form or as an intramuscular injection.
Transdermal estradiol patches are the gold standard when it comes to treating women who are at high risk of a venous thromboembolic event. It simply does not increase the risk of developing a venous thromboembolism. The only thing you should keep in mind is that patches are not always well tolerated because of the lifestyle changes required to keep them from falling off and the fact that they tend to irritate the skin.
It’s difficult to find hard numbers regarding the relative risk of venous thromboembolic events with regards to hypertension. The best I could find after an hour or so of searching was this study regarding VTE in lung cancer patients. Hypertension increased the risk by a factor of 1.8.
As far as the anti-androgen is concerned: The primary use for spironolactone for cisgender people is as an antihypertensive.
Even if the risk of thromboembolism was truly significant with modern hormone replacement therapy it wouldn’t justify what your doctor is doing to you. The fact is that mortality in the transgender community from suicide–caused in part due to the lack of access to hormone therapy–is substantial. The quality of life lost when a trans woman is denied hormone therapy is substantial. The fact that your doctor does not appear to be taking this into consideration when they weigh the risk of thromboembolism against not receiving necessary medical care is deeply concerning.
I strongly recommend that you seek a doctor who is more sensitive to your medical needs as a transgender woman.
Edit: Fixed a minor, but embarrassing, error.
oh wow this is so helpful & good info
Everyone who cares about transfem people please reblog this
this was really fucking helpful
I know a lot of trans women dont have acess to information like this and its very helpful.
Here’s some stuff I could have used being told when I started HRT:
If you do HRT, you are seizing control of and reconfiguring an aspect of your own metabolism, which is fucking cool and amazing, but despite what medical literature and community knowledge exists, you must always be your own advocate in the process (even if you think you have good doctors). As someone who deals with hypervigilance, I’m not going to tell anyone to be more vigilant, but HRT has myriad and subtle impacts on your body and mind (duh). Some of these you probably want, some of these you probably don’t, but telling the difference can be more tricky than you think.
Really watch yourself for side effects. I don’t mean relatively rare side effects like liver damage or blood clots, but simpler stuff that’s much easier to dismiss as just being transient or bearable, like nausea or mood swings. Such side effects are likely to be be small and easy to deal with in the beginning, easily borne, but if they become more serious over time they can do so so slowly that you don’t realize your quality of life is being reduced, especially if you’re loving many of the effects of HRT at the same time. Don’t accept any side effects of your meds as unavoidable, or akin to a price you have to pay for HRT’s benefits. Just adjusting the dosage of your meds, the times you take them, how you take them, and what you take them with can have a huge impact, but doctors can leave out that this is a process of experimentation, and that finding the right combinations of meds and dosages can take time.
Evangelical is not a word I ever thought I’d use for myself, and I’ve only been on bicalutamide for a week, but wow. If you are using spiro and experience any nausea or stomach pain while on HRT, even if you think it has other causes, or if you’re someone like me who carries their anxiety or fear in their stomach, I’d highly suggest at least trialing bicalutamide in place of spiro, just to make sure you know what’s causing that pain and/or nausea. I took 300 mg/day of spiro for about a year, and was waking up in pain and nausea every day without connecting the dots. Now that I’ve switched anti-androgens and tapered off spiro, in just a week I have twice the appetite and almost no stomach pain. What pain I do have dimishes every morning. So far, bica has been literally life-changing for me.
But I only found out about bica from another trans woman, here on tumblr ( @social-justice-cleric ) . My doctor insists he mentioned it as an alternative, more than a year ago, but frankly he stood by as my stomach pain became worse and worse, and only switched me to bica when I did my own research and asked him to. Don’t underestimate the importance of community and its accumulated knowledge- make sure you find other trans people you can talk about your transition without fear of judgment, especially including talking about any and all biomedical components of it. This is especially important for trans women who tend to socially isolate ourselves in response to stress or uncertainty (aka, me).
And as someone who really wanted results from HRT as quickly as possible, it’s ok if you end up wanting to step back your dosages, or if a medication doesn’t work out. This should seem obvious, but it doesn’t make you less of a woman to slow down or even stop doing HRT. Additionally, don’t assume that the speed at which your appearance changes is necessarily correlated to the amount of meds you take- there is for everyone a threshold of dosage past which there is no benefit (and instead just increased risk). For instance, I just finished a two month trial of progesterone- maybe my breasts developed a little more than they otherwise would have, but mostly I just had slight mood swings that trended slightly more to the negatives than the positive, so I’m not going to keep taking the stuff. And if spiro was the only anti-androgen out there, I might have stopped taking one entirely rather than stay on it. But decisions like these are hard, and intensely personal- your doctor can’t, or at least shouldn’t, make them for you.
Ultimately, all the biomedical means of transitioning are for is getting the changes you want to your body and/or mind. And despite the legal-functionary and regulatory components of biomedical transistion, these means do not make you into a woman. Regardless of whether or not you apply these biomedical technologies to your own transition, you are a woman. Some of us trans women come to accept increased medical risks, or endure physical discomfort, in pursuit of the self and life we want. In this, we are hardly alone among women. And, as is the case for any patient heading into a doctor’s office, what medical experts tell us must always be judged against our own embodied expertise.
Biomedically transitioning shouldn’t be seen as a necessary stage of one’s gender transition- it should be an opportunity available to all of us, but not one we all must take, or need to take, to be happy. Since we live in such a cissexist and transphobic society, biomedically transitioning is for many of us a desperately needed means of survival. And at the same time, and in equal measure, it is also for many of us a source of incredible joy. Listen to your doctor, listen to the community, listen especially to your body and to your own heart, and see what works for you.
Also, as a trans woman who has a chronic liver disease, bicalutamide can be hepatotoxic (damaging to the liver) and so far Spiro is the safest antiandrogen if you are a trans woman or AMAB nb in a similar situation as me. However, bicalutimide has not been tested in hrt doses, which are much smaller than the doses bicalutimide was originally for. Feminization begins as low as 12.5mg and the doses tested were 150mg.
estradiol depot is good replacement for valerate as well. 2nding the injections over pills. you can get so much more estrogen into your system SAFELY when it doesn’t have to be processed by your liver (which is what pills have to do).
It seems like a lot of this advice would be useful to anyone considering or taking HRT – man, woman, or enby. And absolutely, always be your own advocate. Your health is ultimately in *your* hands, not those of your doctor.
1. DEMAND condom use 2. Hold your partners accountable for what happens in the bedroom. None of this “baby I can’t control myself around you” or “I just wanted you so bad” bullshit. 3. Coercion is real and it’s very scary and hard to identify in the moment. Establish a dialogue with your partner. Be clear on what you both want. Be clear on what you don’t want. Your boundaries should ALWAYS be respected. 4. Sex can be really emotionally and physically over-stimulating the first few times; don’t be afraid or ashamed to ask your partner to slow down, take a break, or even stop. 5. Focus less on pleasing your partner and more on exploring your partner. Everyone’s body is different and there are no “tricks” to better sex. Chances are, if you psych yourself out worrying over how well you’re “performing” then nobody’s going to have a good time. 6. Ask questions, offer suggestions. Despite what porn has probably taught you, talking during sex isn’t weird or taboo. Your partner isn’t a mind reader. They don’t know what feels good to you. [Pro-tip, a looot of people without clitorises aren’t fully aware of just HOW sensitive a clitoris is. They can be a little rough with them. Tell them to chill!!!!] 7. Your sex life is YOUR business. Don’t ever feel ashamed of how many or how few sexual partners/experiences you’re having. Do what you want, touch the people who want to touch you back, forget the rest. 8. DON’T FAKE YOUR ORGASMS!! Don’t fake your orgasms!! DON’TFAKEYOURORGAMS!! If your partner isn’t getting you there, let them know! Tell them how!! 9. There is more to sex than orgasms. Sex is a really cool way to establish intimacy and trust, to have a fun time, to relieve stress, to explore a person’s body and bring them pleasure. Don’t get me wrong, orgasms are really cool and good, but your sex life is going to be a lot better if it doesn’t revolve around them. 10. LEARN ABOUT YOUR BODY!! This goes for everyone, but ESPECIALLY if you are a person in possession of a vulva, you have been discouraged and even actively kept from vital knowledge about your anatomy! Do some google searches, buy a human sexuality textbook, masturbate. 11. Virginity is a useless concept. It’s completely okay if your virginity is something important to you and I’m not trying to belittle that idea. Just, for the record, in the grand scheme of things it’s not a big deal. Literally nothing about you changes just because you bumped uglies with someone else.
This has been a public service announcement from your friendly internet poet.
Talking about sex when not being sexy is the best first step to having sex. Don’t talk about it to turn on your partner, just discuss it casual. Talk about your thoughts and feelings, what you think you want, what scares you, what interests you, etc. Like anything you can think of. It makes the act easier and can help you establish boundaries before the act starts. Try doing it on a phone or over text so you know sex won’t start. Sometimes the distance helps you be honest.
i like how positive this post is and how it isn’t gender specific <3 <3 <3
Some solid stuff here!
Also: no matter what genitals you have or what you’re doing, a little lube can go a LONG way and even be the difference between if sex will even happen or not. It’s nothing to feel embarrassed about asking for, and even if you’re not sure you’d need it, it might make the experience more enjoyable faster than it would without.
And don’t neglect to clean up afterward!! This is really important, too.
I’d like to add don’t worry if your virginity someone who turns out to be a jerk or wasn’t the special experience you expected or wanted.
This does not define you or your sexual journey and it is so common you’re not weird for having a less than great first experience.
To be perfectly honest even with the ‘right’ person your first time will most definitely suck, sexually, it’s all the times after getting to know what you and your partner like that is the best part.
p.s. also getting to point where your comfortable enough with your partner to roll around crying laughing when they fall of the bed cos it will happen mid-sexy times.
as someone who has a really bad experience with her sex life, follow these advices. they are completely true and important to take in mind <3
Also, from one person with a vagina to any others: not everyone bleeds the first time AND bleeding can happen any time you have sex or sexy alone times involving penetration.
Here [x] is a list of reasons it may happen and suggestions about how to proceed–a lot of times it’s simply because of friction, which is why the point about lube is very important. Some of us learn these things the hard way and think we’re marked for death, but you’re most likely okay! Proceed with caution, but don’t freak yourself out.